
 Bupropion is a norepinephrine and Tesofensine withdrawal symptoms dopamine reuptake prevention that is made use International shipping of Tesofensine for depression and cigarette smoking cessation therapy. It activates pro-opiomelanocortin (POMC), a neuropeptide that reduces appetite when its concentration raises in the hypothalamus, and supplements dopamine activation, which is lower among patients with weight problems. Because of this, bupropion hinders food intake using the incentive system and raises power expense for weight decrease [23] Naltrexone is a mu-opioid receptor villain that is made use of for the treatment of opioid-and alcohol-dependence. Naltrexone prevents the appetite-enhancing results of beta-endorphin triggered by cannabinoid-1 receptor activation. The combined use bupropion and naltrexone has a collaborating impact on hunger suppression [24– 26]
Bupropion is a norepinephrine and Tesofensine withdrawal symptoms dopamine reuptake prevention that is made use International shipping of Tesofensine for depression and cigarette smoking cessation therapy. It activates pro-opiomelanocortin (POMC), a neuropeptide that reduces appetite when its concentration raises in the hypothalamus, and supplements dopamine activation, which is lower among patients with weight problems. Because of this, bupropion hinders food intake using the incentive system and raises power expense for weight decrease [23] Naltrexone is a mu-opioid receptor villain that is made use of for the treatment of opioid-and alcohol-dependence. Naltrexone prevents the appetite-enhancing results of beta-endorphin triggered by cannabinoid-1 receptor activation. The combined use bupropion and naltrexone has a collaborating impact on hunger suppression [24– 26]
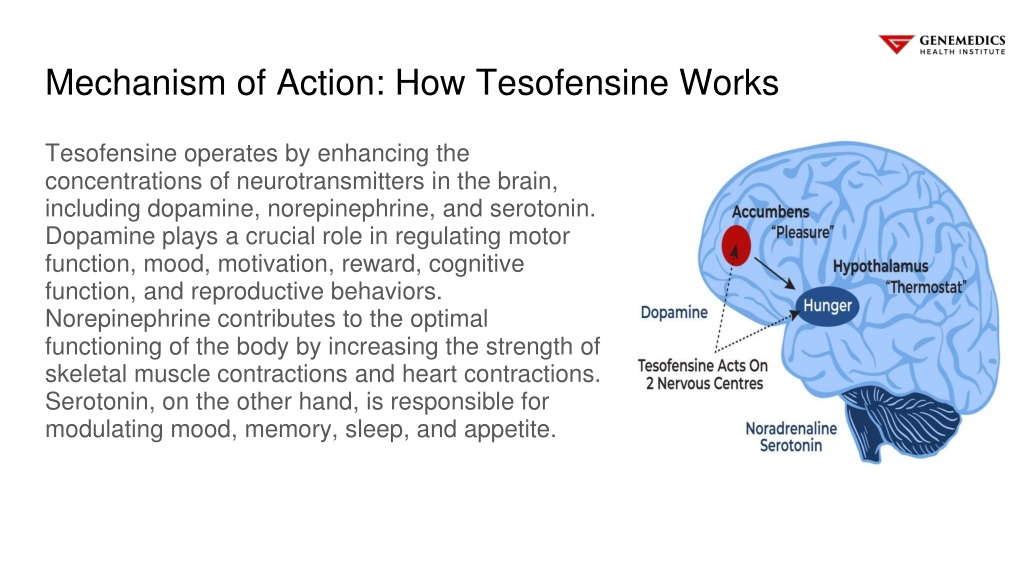
This impact contributes to fat burning by’creating a calorie deficiency and allowing the body to melt even more calories than it consumes. Tesofensine’s synaptic result can bring about serious psychiatric events (anxiety, panic attacks, state of mind conditions). Tesofensine is a prevention of noradrenaline, dopamine and serotonin reuptake that is likewise reported to indirectly boost the cholinergic system(Thatte,
 Sores in the LH can create reduced food consumption and weight-loss, while stimulation can enhance food consumption and advertise excessive weight [6, 7] The LH consists of two major neuronal populations, GABAergic and glutamatergic neurons, that play opposing and bidirectional duties in benefit and feeding [8– 10] In computer mice and primates, activation of LH GABA nerve cells promotes food consumption, while silencing them inhibits food consumption [11– 13]
Sores in the LH can create reduced food consumption and weight-loss, while stimulation can enhance food consumption and advertise excessive weight [6, 7] The LH consists of two major neuronal populations, GABAergic and glutamatergic neurons, that play opposing and bidirectional duties in benefit and feeding [8– 10] In computer mice and primates, activation of LH GABA nerve cells promotes food consumption, while silencing them inhibits food consumption [11– 13]
Egan’s analysis indicated that the drug increased a patient’s threat of issues like anxiety, depression, aggression, and psychosis, while various other data showed a surge in suicidality, including 3 suicides during medical research studies, according to the Times. Arise from a medical trial showed that weight-loss with Tesofensine pharmacodynamics peptide was considerably higher over a six-month period than those attained with any one of the medications currently available. Fat burning depended on 10.6% in patients, which was around two times the fat burning generated by medicines currently approved by the United States FDA for dealing with excessive weight. We make use of dental tesofensine peptide, the latest game-changing peptide established for the therapy of weight problems, as one of our techniques.
Surprisingly, DeepLabCut evaluation introduced for the very first time that phentermine-treated rats displayed less onward mobility than control rats (in spite of it being an energizer drug; Fig 7A). Especially, International shipping of Tesofensine phentermine induced solid head weaving stereotypy, which boosted progressively over 7 days and inhabited 80% of the time of the 4-hour session (Fig 7C). Head weaving stereotypic habits involved rats stalling on 4 legs and relocating their head unpredictably (S4 Video clip), gone along with by frequent uncontrolled tongue movements (although we did not formally evaluate tongue activities, we report them as a subjective human visual monitoring). The beginning of stereotypy decreased from 56.1 ± 23.2 mins on the initial day to 5.5 ± 1.8 minutes on the seven days of therapy (Fig 7D). After showing the anorexigenic results of tesofensine in lean Vgat-ChR2 mice, we intended to replicate our findings in obese Vgat-IRES-cre computer mice.
Box 1 Endocrine Control Of Food Intake
This efficacy is higher than for presently approved single excessive weight drugs, however the altitudes in high blood pressure and heart price are a reason for issue and led to discontinuation of growth. Notably, phase II outcomes for two unimolecular, long-acting GIPR/GLP1R co-agonists have been reported. The very first, NN9709 (previously MAR709 and RG7697) (Table 2), is fit for once-daily subcutaneous injection and demonstrates well balanced high strength at human GLP1R and GIPR193. NN9709 lowered blood glucose, body weight and total cholesterol in a 12-week phase II research of T2D as compared to placebo193. Nonetheless, the improvement in body weight was not statistically various about dose-titrated liraglutide.
A Globally Yearly Study Of New Data In Unfavorable Drug Reactions
Particularly, GLP1R and GIPR agonists enhance glycaemia via their capacity to boost insulin secretion130 and by preventing gastric emptying to reduce sugar access to basic circulation131. Individual demographics and baseline attributes in a randomized scientific trial of Tesomet for hypopituitary people with hypothalamic excessive weight. No statistically considerable distinctions using Pupil’s t-test for continuous variables or Fisher’s specific examination for categorical variables were discovered.
In the 1950s and 1960s dexamphetamine was commonly suggested for a variety of issues consisting of weight problems, depression, and inadequate inspiration (Kiloh and Brandon, 1962). Although it was identified that it might sometimes be taken as a practice to recover self-confidence it was usually thought about safe also for long-lasting use (Editorial, BMJ, 1955). Nonetheless, it came to light that some people were abusing dexamphetamine and had been fraudulently acquiring multiple prescriptions and having them dispensed by different pharmacies (Kiloh and Brandon, 1962). A couple of were admitted to hospital with psychosis and lack of nutrition, experiencing depression on medicine withdrawal. Then the point of view suddenly turned against the stimulants for the treatment of obesity (USA Fda, 2012). Despite this, the stimulant phentermine has actually remained to be licensed for short-term usage in obesity and in combination with the anticonvulsant topiramate for long term usage.